









by Maxime Sermesant (Inria and Université Côte d’Azur)
With medical imaging’s ability to provide a high level of detail about cardiac anatomy and pathology, it is high time for such information to be used during interventions. Technology to achieve this is now being made available to every cardiologist.
Ventricular fibrillation is a pathology in which cardiac electrophysiology, which controls the contraction of the heart, deteriorates into chaotic behaviour. The electric wave that has to activate each muscle fibre of the heart in a coordinated way becomes a storm that does not generate an effective contraction, a condition that is deadly within minutes without heart massage and defibrillator. This sudden death affects 400,000 people a year in Europe, which is more than the three most deadly cancers combined.
The occurence of ventricular fibrillation depends largely on the extent of myocardial infarction: when it is not fatal, it produces damage that can cause arrhythmias years later, such as fibrillation or tachycardia. Traditionally these are treated by implanting a defibrillator, which will trigger an adequate electric shock in case of arrhythmia. But this does not heal anything, represents a major intervention, and the electric shocks often affect the individual’s quality of life.
In recent years, another intervention has been developed, catheter ablation, which allows the cardiac cells responsible for arrhythmias to be burnt with a catheter. However, it is a complex procedure because the cardiologist only has access to a very compartmental vision of the heart during these interventions and must therefore exhaustively search for the right targets.
Medical imaging nowadays, however, makes it possible to obtain, in a non-invasive way, very detailed 3D information on the anatomy and the cardiac structure of these patients. Magnetic resonance imaging and computed tomography now have spatial resolutions of the order of a millimetre. But these data are not currently available to the interventional cardiologist. The acquired images are interpreted by the radiologist and the cardiologist receives a report, but the 3D data cannot be used by the catheter systems.
A new technology developed between Inria Sophia Antipolis and the IHU Liryc in Bordeaux makes it possible to extract the important information from the 3D images of the patient's heart and to represent them in the form of meshes compatible with the interventional tools. The cardiologist can therefore manipulate his catheter while visualising the locations of the sensitive structures to avoid, and the areas to aim for. This accelerates the process, improves safety and increases the success rate [1]. This technology has been tested on hundreds of patients around the world and has been transferred to the start-up company inHEART, created in 2017 to commercialise this tool [L1].
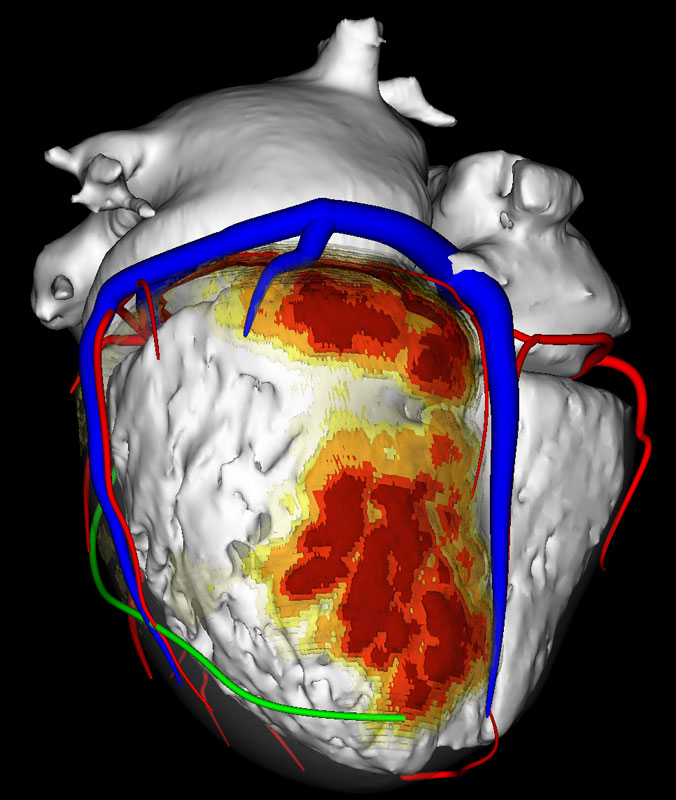
Figure 1: 3D rendering of the cardiac atria and ventricles (white), veins (blue), coronaries (red), phrenic nerve (green) from CT and fibrosis quantification (yellow to red) from MRI. This detailed information provides structures to avoid (vessels, nerves) and areas to treat (fibrosis) when performing catheter ablation of arrhythmias.
However, to implement this technology, it was necessary to tackle various scientific and technical challenges:
- It is necessary to develop robust and fast image processing algorithms. Speed is required to integrate into the clinical workflow without adding additional time. Robustness is crucial for the results to be relevant even in difficult cases, for example if the image is of lower quality. The validation / correction step by the user must not take too much time compared to the time it would take to do everything manually, otherwise the algorithm loses its relevance.
- A key step is segmentation, which extracts important structures from the image. This is one of the major steps because the accuracy of the information provided to the cardiologist depends on it. The method used is based on deep learning [2] but allows the user to correct the result and validate it.
- It also requires image registration algorithms, which allow the matching of information from several modalities, such as MRI and CT. MRI can be used to image fibrosis and therefore the result of infarction, but not small structures such as coronaries, while CT does it very well. The ability to merge these modalities allows a more complete vision of the heart. Again, there are automatic techniques, but it is important to obtain the robustness necessary for clinical use, and that the user can guide the algorithm, including points of interest in each of the images.
- In addition, these algorithms must be integrated into software that can be used by a non-specialist, because in order to allow wide-scale use, the end-user must not be a specialist in medical imaging, nor a radiologist or a cardiologist. This is an ergonomic challenge so that the sequence of steps is natural [L2].
- Finally, we must develop an intuitive visualisation of the different meshes generated because they will be added to the substantial existing data that the cardiologist will have to interpret during the intervention. We are not all equal in 3D visualisation, and the results must not be confusing, so it is important to interact with cardiologists to optimise this aspect.
On these different aspects, the contribution of computing is crucial, and the scientific challenge is notably to succeed in making the algorithms work on images coming from any hospital in the world, with different acquisition protocols and very variable image qualities.
A related area of research is the mathematical modelling of the heart, which could non-invasively predict ablation targets by simulating different electrical propagations and ablation strategies before the procedure. This is also part of the collaborative scientific program between IHU Liryc and Inria and is based on the image analysis outlined above. The challenge here is to succeed in quickly and robustly customising such mathematical models to a patient's images in order to generate the corresponding predictions [3].
Computer science allows this convergence of domains (imaging, modelling, catheters) and thus creates new and exciting possibilities for improving the success and safety of cardiac procedures.
Links:
[L1] https://www.inheart.fr
[L2] https://team.inria.fr/epione/en/software/music/
References:
[1] S. Yamashita, H. Cochet, F. Sacher, S. Mahida, B. Berte, D. Hooks, J.-M. Sellal, N. Al Jefairi, A. Frontera, Y. Komatsu, H. Lim, S. Amraoui, A. Denis, N. Derval, M. Sermesant, F. Laurent, M. Hocini, M. Haissaguerre, M. Montaudon, P. Jais: “Impact of New Technologies and Approaches for Post-Myocardial Infarction Ventricular Tachycardia Ablation During Long-Term Follow-Up”,Circulation - Arrhythmia and Electrophysiology, 9(7), 2016.
[2] S. Jia, A. Despinasse, Z. Wang, H. Delingette, X. Pennec, P. Jaïs, H. Cochet, M. Sermesant: “Automatically Segmenting the Left Atrium from Cardiac Images Using Successive 3D U-Nets and a Contour Loss. In Statistical Atlases and Computational Modeling of the Heart (STACOM”), LNCS, Springer, 2018.
[3] N. Cedilnik, J. Duchateau, R. Dubois, F. Sacher, P. Jaïs, H. Cochet, M. Sermesant: “Fast Personalized Electrophysiological Models from CT Images for Ventricular Tachycardia Ablation Planning”, EP-Europace, 20, 2018.
Please contact:
Maxime Sermesant
Inria and Université Côte d’Azur, France
+33 4 92 38 78 11

