









by Fulvio Patara and Enrico Vicario (University of Florence)
The RACE project (Research on Evidence-based Appropriateness in Cardiology) exploits innovative infrastructures and integrated software services with the aim of “providing the right care, to the right subject, at the right time, by the right provider, in the right health facility”.
Appropriateness in medicine is the proper or correct use of health services, products and resources [1]. To evaluate and support appropriateness, ICT plays a crucial role, offering a growing ecosystem of medical diagnostic and health monitoring devices, communication networks, health information systems, and medical data analytics. In this scenario, data and service integration is key to overcoming issues resulting from heterogeneous insular systems (i.e., information silos) and data with high complexity in terms of volume, variety, variability, velocity, and veracity.
The RACE project [L1] fits into this context with the challenging goal of designing and developing a hardware/software architecture for effective implementation of more personalised, preventive, participatory, and predictive models of continuity of care (i.e., P4-medicine) from hospital to home. A prototype of the overall architecture has been tested over a concrete operative scenario, demonstrating its applicability in the remote monitoring of patients with chronic moderate heart failure (NYHA class II-III). We illustrate here some core concepts of the proposed architecture, focusing on the specific contribution of the University of Florence in the design and engineering of Empedocle [2], an Electronic Health Record (EHR) system characterised by adaptability and changeability as primary requirements.
The RACE architecture for continuity of care
RACE is an architecture-driven project for remote patient monitoring whose components can be organised in three main layers, as shown in Figure 1.
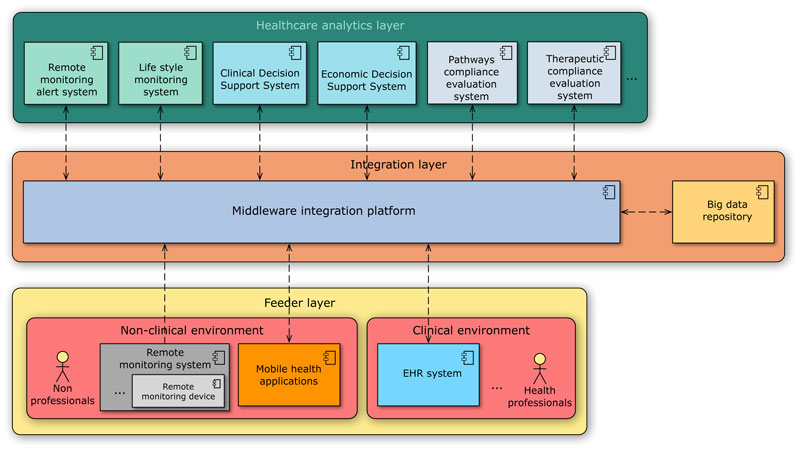
Figure 1: Overview of the RACE architecture.
Feeder layer – This level is characterised by HW/SW systems used by healthcare professionals within clinical settings, or by non-professionals in non-clinical environments, for tracking the state of a patient across time. On the one hand, EHR systems serve as a key instrument for recording, retrieving and manipulating repositories of health information in computer-processable form within clinical environments. On the other hand, remote monitoring devices comprise a primary source of information for health status monitoring of patients in non-clinical settings (e.g., home), particularly in the management of chronic diseases. They typically require sensors to measure specific physiological parameters (e.g., blood pressure, heart rate, pulse oximetry) and wirelessly communicate to a gateway connected to the Internet, so as to feed the architecture with acquired data. Mobile health applications running on portable devices can integrate raw sensor data with higher information provided by non-professionals in order to support patient self-management by improving treatment adherence and offering automated medication reminders and alerts on out-of-range measurements.
Integration layer – Continuity of care gives emphasis to the semantic interoperability between multiple sources of information deployed on different settings. To ensure a real integration of data (produced by the feeder layer) and services (exposed by the healthcare analytics layer), the proposed architecture exploits a middleware integration platform for implementing loosely-coupled publish-subscribe communications between independently deployed and heterogeneous systems over a bus-like infrastructure. All moved clinical events are stored in a centralised big data repository that contains the full medical history about patients.
Healthcare analytics layer – A variety of data analytics systems are built on top of this architecture with the aim of processing historical records or new information stored in the big data repository for real-time and ex-post analytics uses. They are organised in three main categories based on their specific goals. Monitoring systems examine sensored data and generate personalised reminders for patients, and alarms for healthcare professionals in the case of adverse measurements. Decision Support Systems (DSS) assist clinical decision-making tasks (i.e., clinical DSS), as well as giving economic indicators to compare the costs and health outcomes of alternative care pathways (i.e., economic DSS). Finally, compliance evaluation systems evaluate the appropriateness of therapeutic treatment choices and care pathways.
Empedocle in action: an adaptable EHR system for continuity of care
The integration of multiple sources of structured information and the involvement of a variety of actors with different expertise emphasise the responsibility of EHR systems, which become key components in driving the patient to specific care pathways and, subsequently, in remotely monitoring the evolution of the patient’s health status. In this context, we have developed the Empedocle EHR system [2], a J2EE web-application that exploits a two-level meta-modelling architecture based on the Reflection architectural pattern [3] to combine the expected commodity level of any EHR system with some specific requirements posed by a real operative scenario of continuity of care, as: agile adaptability of the EHR data structure to different organisational contexts; interoperability of data and services across the platform; usability by users with different specialty expertise.
In such a scenario, Empedocle becomes a powerful real-time monitoring dashboard, offering to health professionals an effective alternative to in-clinic follow-ups, achieved by the integration of remote monitoring data in the local adaptable EHR. Moreover, the service orchestration capabilities offered by the integration platform enable several existing services to work together for enriching the EHR with higher-level knowledge (e.g., diagnostic investigations, drug interactions, contraindications, etc. as recommended by clinical guidelines implemented by the clinical DSS). Given the variety of skills involved in the process, connecting data with guidelines represents a key aspect for improving patient safety, reducing clinical risk, and evaluating the appropriateness of care.
The RACE Consortium
RACE was co-fonded by Tuscany Region (Italy) in the POR FESR 2014-2020 program from June 2015 to September 2018, and composed by industrial partners (i.e., GPI Group, Codices, Kell, Medilogy, Spinekey, TD Nuove Tecnologie), public health institutes (i.e., G.Monasterio Foundation, Institute of Clinical Physiology of Pisa, Careggi University Hospital) and universities (i.e., University of Florence, Sant’Anna School of Advanced Studies).
Links:
[L1]: https://stlab.dinfo.unifi.it/race-project
References:
[1] Canadian Medical Association. “Appropriateness in Health Care”, 2015.
[2] F. Patara, and E. Vicario: “An adaptable patient-centric electronic health record system for personalized home care”, in Proc. ISMICT, 2014.
[3] F.Buschmann et al.: “Pattern-oriented Software Architecture: A System of Patterns”, 1996.
Please contact:
Fulvio Patara, University of Florence, Italy
Enrico Vicario, University of Florence, Italy

