









by Christophe Ponsard and Renaud De Landtsheer (CETIC)
Within a medical setting, clinical pathways enable efficient organisation of care processes, which benefit both the patient and hospital management. Digital health analytics plays a critical role in the successful deployment of clinical pathways. Two key aspects learned from our experience are the engineering of accurate workflow models and the use of online schedule optimisation, enforcing both care and resource constraints.
A clinical pathway is a multi-disciplinary view of the care process for a group of similar patients suffering from the same disease and with predictable evolution [1]. While scheduling the care for a single patient is straightforward, scheduling the care for a group of patients, and under limited resources is much more complex. Operating clinical pathways is very challenging because of the need to achieve the timely delivery of treatments like chemotherapy. It also requires a thorough knowledge of the history of each patient. Typical care quality indicators monitor the deviation from the ideal pathway and studies have stressed their correlation with cancer survival rate. Moreover, the actual workflow might be quite different from the defined workflow owing to adaptations resulting from a multidisciplinary context and the high level of personalisation.
Within the PIPAS project [L1], together with the Université catholique de Louvain, we have been engineering such a pathway. We started by developing a toolbox supporting the modelling and optimal scheduling of complex workflows [2]. To engineer medical process models, we defined and implemented different operators to combine/distinguish specific treatment for multi-pathology patients and to provide global or more focused viewpoints for specific agents (e.g. patient, nurse radiotherapist) or clinical departments.
Workflows of this kind need to be enacted precisely in order to ensure high quality of care to the pool of patients given the available resources (e.g. staff, beds, drug stocks). In order to orchestrate the work of a oncology day hospital, we developed an online scheduler dealing with the appointments and global nurse and room allocation [3]. Based on all the inputs illustrated in Figure 1, our tool provides prescriptive analytics capabilities to the nurse in charge of setting appointments, i.e. it will help identify the next appointment date by looking at the time window allowed by the patient care indicator. Il will also minimise impacts on other patients by using a global view on the whole pool of known or even expected patients over their whole treatment period. Each deviation, such as a partial treatment or no show, is also immediately considered and recomputed using an efficient constraint local search engine called OscaR.CBLS [L2]. The scheduler also ensures a smoother repartition of the workload and triggers an alarm if insufficient resources are provisioned. Figure 2 shows how the scheduler can maintain a high care quality indicator (>90 %) until the service load becomes unmanageable.
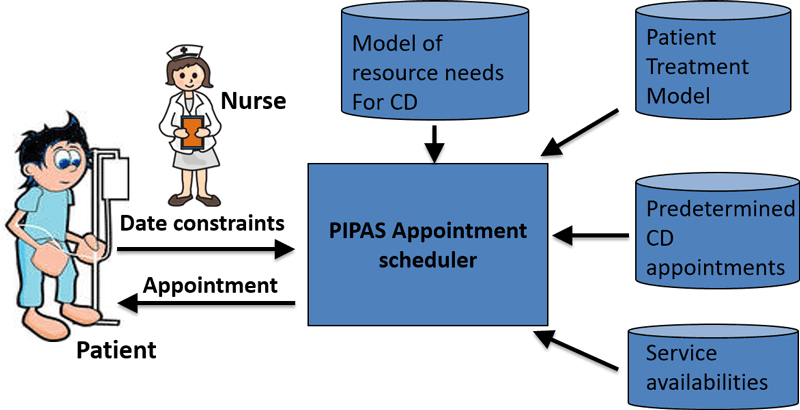
Figure 1: Prescriptive appointment scheduler.
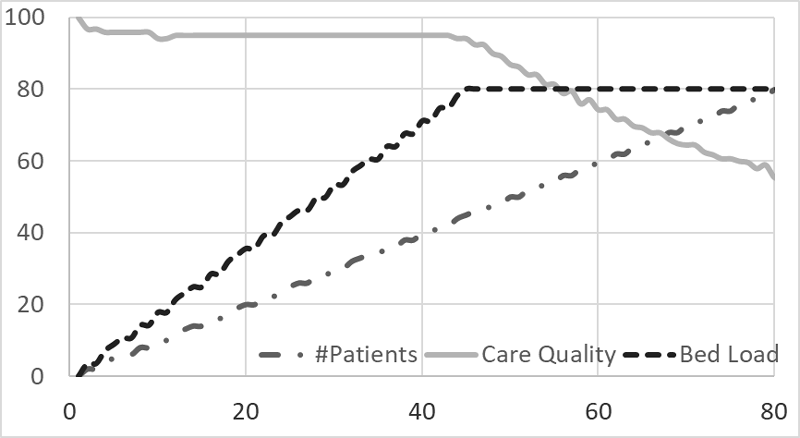
Figure 2: Simulation of service behaviour with increasing patient load until service saturation.
The fact that the actual and theoretical workflows differ from one another, impacts the relevance of the proposed guidance. To address this risk, a reconciliation process analyses the path captured in patient health records to detect the presence of extra transitions, measure their relative frequencies and assess the global variability among patients. Predictive data analytics such as data mining are used here. More specific techniques such as process mining can even help in inferring workflows from data. The result can then be used either to feed the tooling with a more accurate model or to reshape the organisation to enforce the wished workflow. This is our current progress and our next step is to start collecting and analysing data from our new Institute of Analytics for Health (INAH) in charge of providing an ethically controlled access to electronic health information based on the Walloon Health Network.
Links:
[L1] https://www.cetic.be/PIPAS-1169
[L2] https://bitbucket.org/oscarlib/oscar
[L3] https://www.cetic.be/INAH
References:
[1] H. Campbell and al.: “Integrated care pathways”, British Medical Journal pp. 133{137 (1998).
[2] C. Damas, B. Lambeau, A. van Lamsweerde: “Transformation operators for easier engineering of medical process models”, SEHC@ICSE, 2013.
[3] C. Ponsard and al.: “Quality of Care Driven Scheduling of Clinical Pathways Under Resource and Ethical Constraints”, ICEIS (Revised Selected Papers) 2017: 162-186.
Please contact:
Christophe Ponsard, CETIC, Belgium
+32 472 56 90 99

