









by Andreas S. Panayides (Sigint Solutions and University of Cyprus), Marios S. Pattichis (University of New Mexico) and Constantinos S. Pattichis (University of Cyprus)
Video compression is the core technology in mobile (mHealth) and electronic (eHealth) health video streaming applications. With global video traffic projected to reach 82 % of all internet traffic by 2022, both industry and academia are struggling to develop efficient compression algorithms to match these unprecedented needs. To the best of our knowledge, this is the first performance comparison of emerging VVC and AV1 video codecs for medical applications.
Video codecs are currently experiencing unparalleled levels of growth driven by unprecedented video traffic demands that are projected to reach 82 % of all internet traffic by 2022 [1]. This growth is facilitated by advances in open-source video delivery protocols, such as Dynamic Adaptive Streaming over HTTP (MPEG-DASH) and WebRTC (Real-Time Communication (RTC)). Most importantly, industry initiatives such as Google’s WebM project (leading VP8/ 9 video codecs development), and subsequent formation of the Alliance for Open Media (AOM) [L1] comprising key industry affiliates, have created a highly competitive environment, investing efforts towards creating the first ever royalty free video codec. In this context, AOM announced the code freeze of its debut encoder, AV1, in 2018, claiming the best encoding performance to date. At the same time, the Joint Video Experts Team (JVET) formed in October 2017 that has undertaken the development of H.265’s successor, termed Versatile Video Coding (VVC), has just released its reference software abbreviated VTM (VVC Test Model) [L2].
In healthcare, video compression is a key enabling technology that is widely used for real-time medical video communications in a mobile-health setting [2], [3]. Application scenarios range from remote diagnosis and care to emergency incidence response, medical education, tele-robotics, and second opinion provision. A plethora of applications further extends to the home setting for assisted living applications. Moreover, video compression is also key in low-bandwidth applications such as remote diagnosis from isolated locations, developing countries, and disaster sites.
The objective of this study was to investigate the compression efficiency of well established (VP9 and H.265 (also termed high efficiency video coding (HEVC)), recently standardised (AV1), and emerging (VVC) video codecs and provide preliminary insights into their applicability in the healthcare domain.
Experimental Setup
The dataset used in this series of experiments consisted of 10 atherosclerotic plaque ultrasound videos with a video resolution of 560x448 at 40 frames per second, with a duration of 10 seconds, and yuv420p raw format (see Figure 1). Selected quantization parameters values for constant quality encoding, typical in video compression performance comparison studies, were {27, 35, 46, 55} for AV1, VP9 and {22, 27, 32, 37} for VVC, HM, and x265, to enable a fair comparison and a wide range of representative bandwidths given the video characteristics. Random access settings involved an intra update every 32 frames, aligned with the specified group of pictures (GOP) level. Default preset parameters available in every video coded were set at RandomAccess for VVC and HM, --good and –best for AV1 and VP9, respectively, and –placebo for x265.
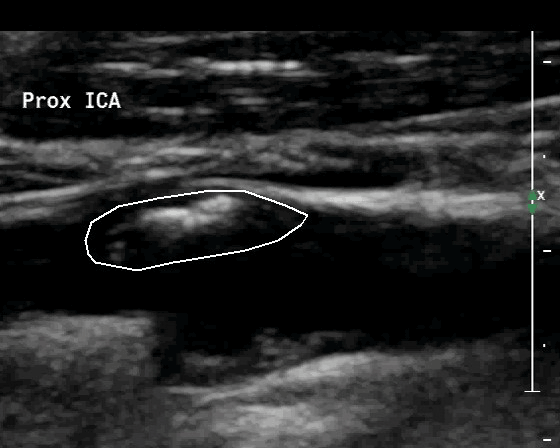
Figure 1: Original (uncompressed) ultrasound video image example of the internal carotid artery (ICA). The straight white line delineates the atherosclerotic plaque causing stenosis. Video resolution: 560 × 448, frame rate: 40 fps.
Performance Evaluation
Preliminary results depicted in Figure 2 and Table 1 show that VVC already appears to outperform AV1, despite VVC being in the early stages of the development process. For this particular experimental setup, bitrate demands reductions of 36 % were recorded for equivalent quality using the BD-RATE algorithm. Interestingly, both HEVC instantiations, namely HM (HEVC Test Model) and x265, demonstrated higher coding efficiency than AV1, with AV1 entailing additional bitrate requirements of 18 % and 4 %, respectively. It is important to note, however, that this finding is largely due to the limited video resolution of the investigated CCA videos. Ongoing experimentation shows that as video resolution increases, AV1 tends to outperform both HM and x265, which is consistent with the published literature. While not obsolete, VP9 is mostly used for benchmarking purposes in this study, significantly lacking in compression efficiency compared to all rival codecs. On a different note, besides x265 and VP9 that involve production level software optimization and hence can qualify for real-time performance, VVC, AV1, and HM incur long compression times, given that their principal intended usage is to validate their compression efficiency rather than for use in real-time video streaming applications.
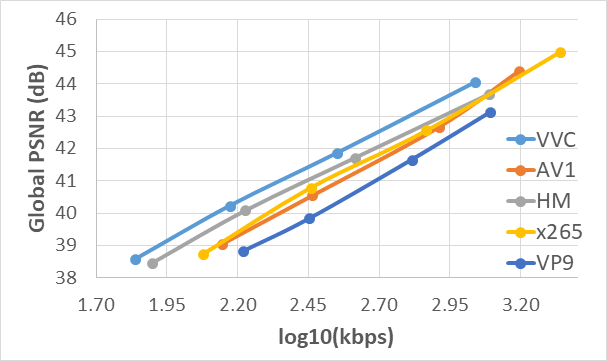
Figure 2: Video coding standards comparison. Rate-distortion curves depicting Peak Signal to Noise Ratio (PSNR) vs log (Bitrate) using mean values of the ten 560x416@40 frames/s ultrasound videos for all investigated QP values. VVC outperforms all rival video codecs.
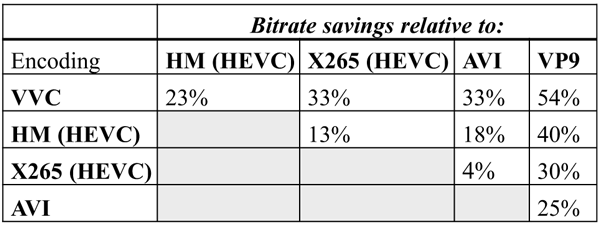
Table 1: Performance comparison of video coding standards in terms of overall bitrate gains. Savings were computed using the BD-Rate algorithm. VVC outperformed all other video codecs.
Undoubtedly, more comprehensive experiments are needed to deduct the best video coding software, investigating different medical video modalities and higher video resolutions (high and ultra-high definition, and beyond). Studies on general-purpose videos in the literature revealed that encoding performance is largely affected by content and video size, and hence safe conclusions can only be drawn once experiments extend across the video resolution ladder and involve a sufficient number of medical video modalities. Such a study is already underway for emergency scenery and echocardiogram videos within the context of the Adaptive Video Control for Real-time Mobile Health Systems and Services (ACTRESS) project.
This work was co-funded by the European Regional Development Fund and the Republic of Cyprus through the Research and Innovation Foundation (Project: POST-DOC/0916/0023); Acronym: ACTRESS.
Links:
[L1] https://aomedia.org/
[L2] https://jvet.hhi.fraunhofer.de/
References:
[1] Cisco, V. N. I.: “Cisco Visual Networking Index: Forecast and Trends, 2017–2022”, White Paper, 2018.
[2] A. S. Panayides, M. S. Pattichis, C. P. Loizou, et al.: “An Effective Ultrasound Video Communication System Using Despeckle Filtering and HEVC”, in IEEE J Biomed Health Inform, vol. 19, no. 2, pp. 668-676, 2015.
[3]: Z. C. Antoniou, A. S. Panayides, M. Pantzaris, et al.: “Real-Time Adaptation to Time-Varying Constraints for Medical Video Communications”, in IEEE J Biomed Health Inform, vol. 22, no. 4, pp. 1177-1188, July 2018.
Please contact:
Andreas S. Panayides
Sigint Solutions and University of Cyprus, Cyprus
+35722892757

